Drug Interaction Mechanism Explorer
Interaction Detected
Risk LevelInteracting Agent
Name of Drug/Supplement
Mechanism Type
Description of the effect.
Clinical Note: Additional context.
Imagine taking two medications that are perfectly safe on their own. Now imagine taking them together, and suddenly they trigger a dangerous reaction in your body. This isn't science fiction; it is the reality of drug-drug interactions, which occur when one medication alters the effect of another. These interactions can turn a helpful treatment into a health hazard, leading to everything from mild side effects to life-threatening emergencies. Understanding how these interactions work is not just for doctors-it is essential knowledge for anyone managing multiple prescriptions.
Every year, millions of people experience adverse outcomes because of unnoticed interactions between their medicines. The good news? Most of these risks are predictable and preventable. By understanding the basic mechanisms-how drugs move through your body and how they affect your organs-you can take control of your medication safety. Let’s break down exactly how these interactions happen, why they matter, and what you can do about them.
The Two Main Types of Drug Interactions
To understand drug interactions, you first need to know that there are two primary ways one drug affects another. Experts classify these as pharmacokinetic interactions, which change how much of a drug is in your body, and pharmacodynamic interactions, which change what the drug does once it gets there.
Pharmacokinetic interactions involve the four steps of how your body handles a drug: absorption, distribution, metabolism, and excretion. Think of this as the journey the drug takes. If Drug A changes how fast your liver breaks down Drug B, that is a pharmacokinetic interaction. The concentration of Drug B might skyrocket or plummet, making it either toxic or useless.
Pharmacodynamic interactions are different. Here, the amount of each drug in your blood stays the same, but their combined effects clash or amplify each other at the cellular level. For example, if you take two drugs that both slow down your heart rate, the result is an additive effect that could drop your heart rate too low. Or, if one drug blocks pain signals and another dulls those signals further, you might become overly sedated.
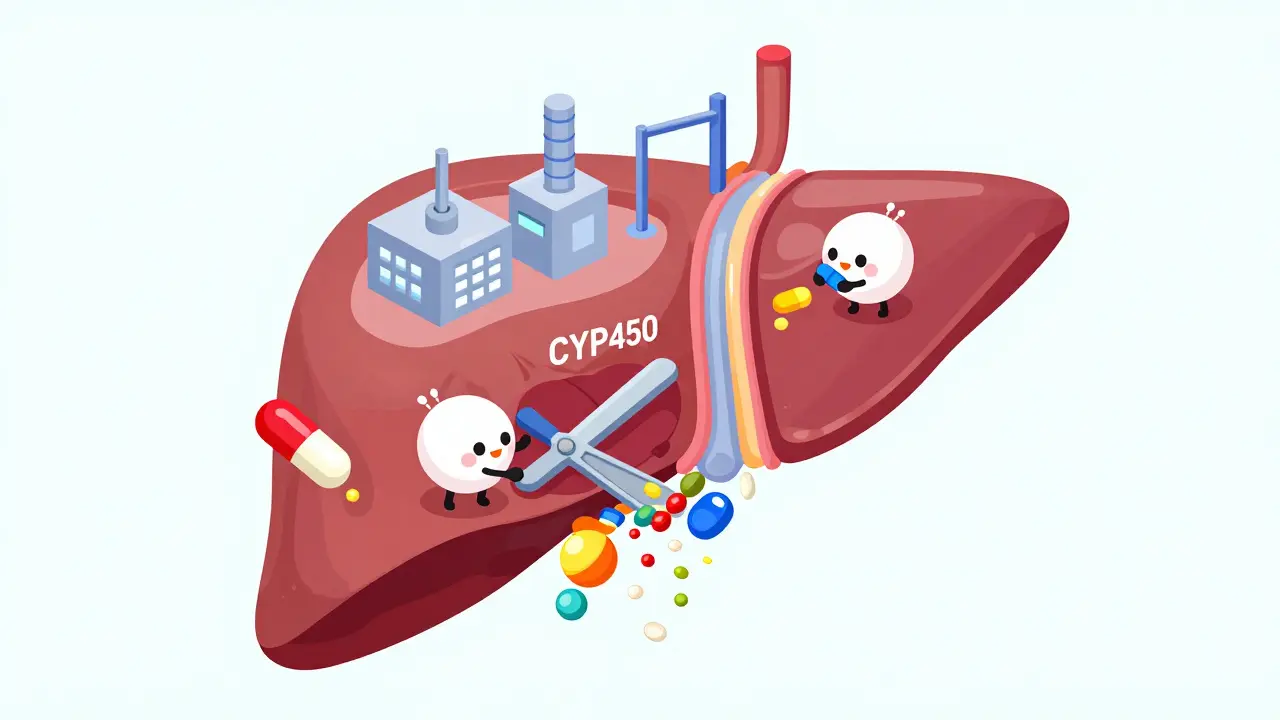
Metabolism: The Cytochrome P450 System
The most common cause of pharmacokinetic interactions happens in the liver, specifically involving a family of enzymes called Cytochrome P450 (CYP450). These enzymes act like molecular scissors, cutting up drugs so your body can eliminate them. About 70% to 80% of all prescription drugs are metabolized by this system. The most important enzyme in this group is CYP3A4, which processes roughly half of all clinically used medications.
Here is where things get tricky. Some drugs don’t just get broken down by these enzymes; they interfere with them. There are two main ways this interference happens:
- Inhibition: One drug blocks the enzyme, stopping it from breaking down the second drug. This causes the second drug to build up in your bloodstream to potentially toxic levels. For instance, ketoconazole, an antifungal medication, is a strong inhibitor of CYP3A4. When taken with simvastatin, a cholesterol-lowering statin, ketoconazole can increase simvastatin levels by 10 to 20 times. This dramatically raises the risk of rhabdomyolysis, a serious condition where muscle tissue breaks down rapidly.
- Induction: One drug speeds up the enzyme, causing it to break down the second drug too quickly. This means the second drug doesn’t reach effective levels in your body. St. John's Wort, a popular herbal supplement, is a potent inducer of CYP3A4. It can reduce the effectiveness of critical drugs like cyclosporine, an immunosuppressant used after organ transplants, by 50% to 60%, potentially leading to organ rejection.
Other key enzymes include CYP2D6, CYP2C9, and CYP1A2. Genetic variations mean some people are "poor metabolizers" while others are "ultrarapid metabolizers," adding another layer of complexity to how these interactions play out in real life.
Absorption, Distribution, and Excretion
While metabolism gets the most attention, interactions can happen at other stages of the drug’s journey too.
Absorption interactions occur in the gut. For example, some drugs change the pH of your stomach or slow down gut motility. If you take a drug that slows digestion, another drug might sit in your stomach longer than intended, altering how much of it enters your bloodstream. Additionally, certain supplements like calcium or iron can bind to antibiotics in the gut, preventing them from being absorbed entirely.
Distribution interactions often involve plasma proteins. Many drugs travel through the blood attached to proteins like albumin. If two drugs compete for the same binding spot, one might get displaced and float freely in the blood. This "free" fraction is the active part of the drug, so even a small displacement can lead to higher active concentrations and increased side effects. Warfarin, a blood thinner, is highly protein-bound and prone to these types of interactions.
Excretion interactions primarily involve the kidneys. Drugs are often pumped out of the body by transporters. If one drug blocks these pumps, the other drug stays in the system longer. For example, verapamil, a heart medication, inhibits a transporter called P-glycoprotein (P-gp). When taken with digoxin, another heart drug, verapamil can increase digoxin levels by 50% to 100%, raising the risk of dangerous heart rhythms.
Clinical Consequences and High-Risk Combinations
Why should you care about these mechanisms? Because the consequences can be severe. Studies show that drug-drug interactions account for approximately 3% to 5% of all hospital admissions among elderly patients. The economic burden is also staggering, with preventable interactions costing the US healthcare system around $1.3 billion annually in direct medical costs.
Some combinations are particularly notorious. The Beers Criteria, a guideline developed by the American Geriatrics Society, identifies over 30 high-risk drug pairs for older adults. Here are a few examples that highlight the danger:
| Drug Combination | Mechanism | Potential Effect |
|---|---|---|
| NSAIDs + Anticoagulants | Pharmacodynamic (Additive bleeding risk) | Increases bleeding risk by 3-5 times |
| Fluoroquinolones + Macrolides | Pharmacodynamic (QT prolongation) | 5.7-fold increase in risk of Torsades de Pointes (fatal arrhythmia) |
| ACE Inhibitors + Potassium-Sparing Diuretics | Pharmacodynamic (Hyperkalemia) | Significant rise in serum potassium, risking cardiac arrest |
| Warfarin + Phenylbutazone | Pharmacokinetic (Protein displacement/Metabolism inhibition) | Severe bleeding due to elevated warfarin levels |
Note that warfarin appears frequently in adverse event reports because it has a narrow therapeutic index-meaning the difference between a helpful dose and a harmful dose is very small. Any interaction that shifts its levels can have immediate, visible consequences like bruising or internal bleeding.

Managing Risks: Tools and Strategies
You don’t have to navigate this alone. Healthcare systems and professionals use several tools to catch these interactions before they harm you.
Electronic Health Records (EHR) now include clinical decision support systems that alert doctors when they prescribe interacting drugs. However, these systems aren’t perfect. A 2022 study found that 80% to 90% of these alerts are false positives, leading to "alert fatigue" where clinicians ignore warnings. Newer systems, like Epic’s "Suggestive Warnings," aim to provide context-specific advice rather than generic alarms, reducing high-severity interaction occurrences by 22% in large studies.
Therapeutic Drug Monitoring (TDM) is another critical strategy. For drugs with narrow therapeutic windows, like warfarin or digoxin, doctors regularly measure drug levels in your blood. For warfarin, the target International Normalized Ratio (INR) is usually between 2 and 3. If you start a new medication that interacts with warfarin, your INR will shift, and your doctor can adjust the dose accordingly.
Community pharmacists play a vital role in prevention. Research shows that pharmacist-led medication reviews can reduce clinically significant interactions by 37%. They look at your entire regimen-including over-the-counter drugs and supplements-to spot potential conflicts that a busy doctor might miss.
Finally, pharmacogenomics is changing the game. By testing your genes, doctors can determine if you are a poor or ultrarapid metabolizer of certain drugs. The Clinical Pharmacogenetics Implementation Consortium (CPIC) provides guidelines for this. For example, if you are a CYP2D6 ultrarapid metabolizer, you might convert codeine to morphine too quickly, leading to toxicity, especially if you are also taking a CYP3A4 inhibitor.
What You Can Do Today
Knowledge is your best defense. Here is how to stay safe:
- Use one pharmacy: Keeping all your prescriptions at one place allows the pharmacist to see your full history and catch interactions automatically.
- List everything: Tell your doctor about every medication you take, including over-the-counter pills, vitamins, and herbal supplements like St. John's Wort.
- Ask questions: When prescribed a new drug, ask, "Does this interact with anything else I am taking?"
- Monitor for symptoms: If you start feeling unusually tired, dizzy, or notice unexpected bruising after starting a new combination, contact your healthcare provider immediately.
- Stay informed: Resources like the Liverpool HIV-Drug Interactions Checker demonstrate how specialized databases help manage complex regimens. While you may not need such specialized tools, general awareness helps.
Drug-drug interactions are complex, but they are manageable. By understanding the mechanisms-from CYP450 enzymes in the liver to P-glycoprotein transporters in the gut-you can engage more effectively with your healthcare team. Your health is a partnership, and knowing how your medications talk to each other is a crucial part of that conversation.
What is the most common type of drug interaction?
The most common type is pharmacokinetic interaction, specifically involving metabolism by the Cytochrome P450 enzyme system in the liver. Enzymes like CYP3A4 process many drugs, and inhibitors or inducers can significantly alter drug levels in the blood.
Can herbal supplements cause drug interactions?
Yes, absolutely. Supplements like St. John's Wort are potent enzyme inducers that can reduce the effectiveness of prescription drugs such as birth control pills, anticoagulants, and immunosuppressants. Always inform your doctor about any supplements you take.
How do I know if I am experiencing a drug interaction?
Symptoms vary widely but may include sudden worsening of side effects, loss of efficacy of a previously working drug, unusual dizziness, excessive bleeding, or extreme fatigue. If you suspect an interaction, seek medical advice immediately.
Why are elderly patients at higher risk for drug interactions?
Elderly patients often take multiple medications (polypharmacy), have reduced kidney or liver function, and may have genetic variations affecting drug metabolism. These factors combine to increase the likelihood and severity of interactions.
Do electronic health records catch all drug interactions?
No, they do not. While EHR systems provide alerts, they suffer from high false-positive rates, leading to alert fatigue. They are a helpful tool but cannot replace careful clinical judgment and pharmacist review.







